
Acoustic Coupling: Fixed vs. Dynamic Venting
Megan Adler, Au.D. and David Taylor, Au.D.
There are many considerations made when fitting hearing aids, which include the style and technology level of the hearing aid, acoustic coupling, the experience level and dexterity of the patient, the types of environments the patient encounters and the importance of streaming audio to the hearing aids. The audiogram may be the most important factor to consider in a fitting, and hearing care professionals (HCPs) know a very common audiogram has good low-frequency thresholds sloping to a high-frequency hearing loss. At first glance, many HCPs would fit the patient with an open earpiece or dome, especially if the person is a first-time user, to ensure good first-fit acceptance. Other HCPs may choose a partially vented or closed coupling to provide benefit in noise and/or improve streaming sound quality. Often there is a compromise between comfort and hearing performance.
Acoustic Coupling and Occlusion
One of the major complaints of hearing-aid users during the hearing aid fitting process is the occlusion effect (Winkler et al., 2016). In fact, according to MarkeTrak VIII data, occlusion is one of the top 10 factors correlated with user satisfaction (Kochkin, 2010). Occlusion can be defined both objectively and subjectively. Objectively, occlusion is the difference in sound pressure level between the occluded and the open ear during self-vocalization. This difference is present primarily at low frequencies. Subjectively, the occlusion effect is the change in perception of the user’s own voice through sealing the ear canal, which can be evaluated via questionnaires or paired comparisons (Winkler et al., 2016).
Ricketts and colleagues (2017) describe the occlusion effect and its origin as follows: during vocalization, sounds can reach 120 to 130 dB SPL or more in the back of the throat, especially during production of vowels. Through bone conduction, these high intensity sounds travel to the mandibular condyle, adjacent to the ear canal. This bone-conducted signal then becomes an air-conducted signal by setting up vibrations of the cartilaginous portion of the ear canal. These vibrations are primarily low frequency. Normally, this energy is allowed to escape out of the open ear canal and does not contribute significantly to our perception of our own voice. However, when an object (such as a hearing aid or earmold) is introduced to the lateral portion of the ear canal, the energy cannot escape, and results in energy being reflected back to the eardrum and transmitted to the cochlea in the typical air-conducted manner.
One of the most important factors governing occlusion is the acoustic mass of the venting. Acoustic mass, also commonly referred to as acoustic inertance, is the effect of inertia in an acoustic system that impedes transmission of sound (ASA, 2016). Acoustic mass can be calculated using the following formula (Beranek, 1954).
Acoustic Mass = Air Density x (Effective Length / Cross-sectional Area)
It is important to think of acoustic mass not as a physical mass, but an inertial property of the system. To better understand the concept, imagine blowing through a drinking straw, a long tubular conduit with a small diameter. This task will require a stronger acoustic force, compared to a paper towel roll. As venting options are adjusted during the fitting process, clinicians are therefore adjusting the impedance of the coupling (and by extension, how well the fitting ‘traps’ low frequencies).
In order to combat an undesirable occlusion effect, a clinician may be inclined to decrease this impedance by decreasing the acoustic mass of the system. By definition, this allows for easier transmission of sound between the residual ear canal volume and the outside environment. Clinicians commonly do this by increasing the vent diameter, decreasing the length of the vent, or using an open dome. Because acoustic mass is calculated as a ratio of length and cross-sectional area, it is possible for a large diameter vent to have equivalent acoustic vent mass as a smaller diameter vent, with a shorter length. When a hearing aid user presents complaints of the occlusion effect, decreasing the acoustic mass of the venting is a viable solution, but it does not come without consequences.
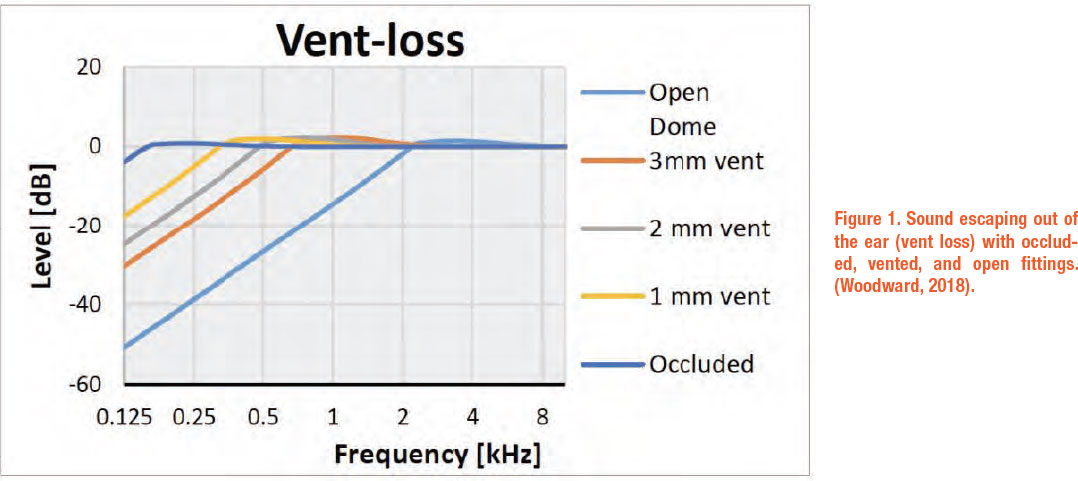
It is important to keep in mind, these adjustments to acoustic mass will not only control how much sound escapes from the ear canal (i.e., ‘vent loss’), but also the amount of direct sound that is able to enter the ear canal. See Figure 1 below for an example of vent loss across different couplings.
It is important to keep in mind, these adjustments to acoustic mass will not only control how much sound escapes from the ear canal (i.e., ‘vent loss’), but also the amount of direct sound that is able to enter the ear canal. See Figure 1 below for an example of vent loss across different couplings.
Considerations of Open Fittings
When open coupling or large venting is utilized, it should be considered how this coupling will create interaction between direct and processed sounds. In the case of open coupling, both direct and amplified sounds are superimposed in the ear canal. When two or more identical audio signals are presented offset in time, it will result in combfiltering. In instances of comb-filtering, frequencies that are in phase are creating a summation effect, and for frequencies out of phase, the signals cancel and result in a notch in the frequency response. Comb-filtering occurs in the higher frequency range, as phase relationships become less correlated when wavelengths decrease in size (Fuston, 2021). Perceptually, the frequency response is altered in proportion to the amount of delay, and this phenomenon elicits an inferior sound quality relative to signals that are in-phase and without any evidence of comb-filtering. Occluded coupling minimizes the transmission of direct sound, thus minimizing the interactions of direct and amplified signals.
Consideration should be made regarding coupling effects on signal processing algorithms. If direct sound is allowed to dominate the amplified signal, the benefit of directionality, noise reduction, and other adaptive algorithms can be reduced (Bentler et al., 2006; Rickets, 2000). Additionally, vent sizes have an effect on compression ratios. Fortune (1997) demonstrated this by evaluating compression ratios measured via real ear measures (REM) for different sized vents, from unvented to a 4.75 mm vent. When the compression ratios were measured via REM, the largest vent had lower compression ratios than the other vent sizes. For modern hearing instruments with wide dynamic range compression, less gain is applied to high input signals, creating more potential for the direct sound to dominate the balance between the amplified and direct signals as input levels increase. These compression effects are important to keep in mind, as the compression specifications in the fitting software may not coincide with the effective compression ratios, or the compression that the user is experiencing in real life, which are inclusive of these venting effects.
Feedback cancellation is also sensitive to venting. Relative to a custom earmold, maximum stable gain before feedback may be reduced by 25 dB with an open dome, and 15 dB with a closed dome (Blau et al., 2008). Feedback reduction algorithms allow for further gain increases but have the potential to produce artifacts and compromise sound quality, so a more closed fitting may be an advantageous approach when managing feedback.
Lastly, it should be considered how open fittings affect perception of non-acoustic inputs. As streaming technology has advanced over the past years and continues to evolve, users will expect a certain degree of performance from these features. In order for a clinician to optimize this experience, the coupling must coincide with the user’s goals. Similarly to how an open fitting will allow for transfer of low frequencies to combat an undesirable occlusion effect, this ability for the low frequencies to escape may elicit an undesirable low-end response when streaming. In many instances, this may be a matter of balancing the user’s goals between reducing occlusion and improving streaming sound quality.
With all these considerations in mind, often times, a hearing aid fitting requires compromise between satisfaction of own-voice perception (occlusion) and maintaining the aforementioned benefits of amplification and signal processing algorithms.
Dynamic (or adaptive) venting
HCPs and patients have become accustomed to digital hearing aids that can adapt their behavior based on the acoustic environment and the (presumed) intent of the user. This adaptive behavior, however, has never included acoustic coupling. As discussed above, an open fitting is better in some ways and a closed fitting in others; often an open and a closed fitting would be ideal for a patient, but switching back and forth between different domes or earpieces isn’t manageable for the average patient, and would make it difficult for the HCP to provide an appropriate prescription.
Recent technological advancements have made a dynamic venting system for hearing aids possible, allowing for a single fitting that can adapt between open and closed venting. Phonak’s ActiveVentTM receiver (compatible with Audéo P-R or P-RT) has a mechanical vent that opens or closes based on the environment or incoming streamed signal. This receiver solves the dilemma that many HCPs experience in the clinic, and now there is no need to compromise between an open and closed fitting.
Benefits of dynamic venting
A patient fit with a ‘fixed’ open fitting would experience a reduced perceived volume level and less full sound while streaming, due to the low frequency energy lost through the vent. In addition, such a patient would suffer from environmental sound entering the vent, interfering with the streamed audio input. Having an open vent in noisy environments is also problematic, because when low-frequency sound escapes the ear canal via the vent, it negatively impacts the directivity of the hearing aid (Ricketts, 2000).
ActiveVent has the ability to switch between the equivalent of a 3.5 mm vent (when open) or completely occluded (when closed). Figure 2 shows the frequency response of the ActiveVent in the open and closed states.
 This dynamic behavior allows patients to avoid some of these negative results of ‘fixed’ open venting by adapting the acoustic coupling between the open and closed vent position to balance comfort and performance. When the vent is open, patients will experience the comfort of their own voice and the natural awareness of environmental sounds in quiet environments. When the vent closes, patients will have a reduced interaction between the amplified signal and direct sound, as well as reduced vent loss, in challenging communication situations. In addition, they will have an improved sound quality of streamed signals compared to a conventional acoustic coupling and an enhanced perception of the streamed signal when ambient noise is present (Latzel & Hobi, 2021; Winkler et al., 2016). Because the vent is not permanently closed, patients can also avoid some of the negative impacts of closed venting, such as the occlusion effect.
This dynamic behavior allows patients to avoid some of these negative results of ‘fixed’ open venting by adapting the acoustic coupling between the open and closed vent position to balance comfort and performance. When the vent is open, patients will experience the comfort of their own voice and the natural awareness of environmental sounds in quiet environments. When the vent closes, patients will have a reduced interaction between the amplified signal and direct sound, as well as reduced vent loss, in challenging communication situations. In addition, they will have an improved sound quality of streamed signals compared to a conventional acoustic coupling and an enhanced perception of the streamed signal when ambient noise is present (Latzel & Hobi, 2021; Winkler et al., 2016). Because the vent is not permanently closed, patients can also avoid some of the negative impacts of closed venting, such as the occlusion effect.
Just as HCPs must learn how to appropriately select and fit ‘fixed’ acoustic couplings, the unique nature of dynamic venting means that some considerations should be taken prior to selection and fitting.
Clinical Considerations
Lifestyle and audiogram
Since a dynamic venting system incorporates both open and closed fittings, the appropriate fitting range of the system will be influenced heavily by the degree of hearing loss appropriate for the open vent condition. In the case of ActiveVent, this includes patients with mild-to-moderate sloping high-frequency hearing loss, who might ordinarily be fit with an open or vented dome. As detailed above, the benefit of the system comes from having closed acoustics when communicating in a noisy environment or while listening to streamed signals, with open acoustics to utilize natural low-frequency hearing in other situations. Therefore, the ActiveVent receiver is ideal for clients who enjoy streaming and are in challenging situations, who might appreciate additional low frequency boost for streamed signals and reduced direct sound interference with the hearing aid signal processing in noisy environments. The patient should also be willing to use a rechargeable hearing aid, since the ActiveVent receiver is not compatible with zinc-air battery models.
Ear Anatomy and Physiology
The ActiveVent receiver can only be housed in a custom earmold (i.e., a SlimTip), and therefore ear canal size and shape may be a limiting factor for some patients. The use of a custom SlimTip helps minimize acoustic leakage when the vent is closed, which helps create the best experience possible. The mechanical switching of the receiver can be adversely affected by wax and moisture, so patients with very waxy ears or known chronic or recurrent middle ear pathologies would not be suitable for ActiveVent. In addition, the ActiveVent receiver is not recommended for clients that report problematic and severe tinnitus and/or reduced loudness discomfort levels, as the change in acoustic output when the vent opens and closes may be bothersome.
Maintenance
The HCP should consider whether a patient’s dexterity will allow him/her to perform regular maintenance of the ActiveVent receiver. Cleaning is important to ensure better daily performance, extend the lifespan of the device(s), and prevents repair issues that can result from wax build-up and moisture. The patient should wipe the hearing aid(s) and earpiece(s) daily with a damp cloth and replace the wax filter(s) weekly.
Hearing aid fitting
When fitting ActiveVent, the vent defaults to open in some programs and closed in others, based on the intended use of the respective program. However, the software does allow for the flexibility of modifying the vent status in various programs. The HCP can also create manual programs with a defined vent state depending on the needs of the patient. This ensures the HCP is aware and in control of the acoustic coupling for the patient in any given program.
When fitting the ActiveVent receiver, the HCP should explain to the patient that there is a vent built within the receiver that opens and closes in response to the environmental sound or incoming streamed signal. The movement of the vent opening and closing creates a sound and is an indication that the ActiveVent receiver is functioning correctly. This sound can be demonstrated to the patient by switching between programs in the software.
Conclusion
Open fittings revolutionized the hearing aid industry by providing a solution for users that experience bothersome occlusion effects. Open fittings also give opportunity to allow direct, natural sound to enter the auditory system, allowing patients with residual hearing in low frequencies to hear naturally. However, open fittings do not come without consequences, such as the undesirable interaction between direct and amplified sounds, negative effects on signal processing algorithms, and reduced sound quality while streaming. Historically, HCPs and patients have had to choose to prioritize either comfort or performance when selecting acoustic coupling. Dynamic venting, like the ActiveVent receiver, allow for comfort and performance to be optimized for a patient with a single device and earpiece. ■
References
- ASA (Acoustical Society of America). (2016, June 3). Acoustic mass. Welcome to ASA Standards. https://asastandards.org/Terms/acoustic-mass/
- Bentler, R., Wu, Y.- H., & Jeon, J. (2006). Effectiveness of directional technology in open-canal hearing instruments. The Hearing Journal, 59(11), 40, 42, 44, 46-47
- Beranek, L.L. (1954). McGraw-Hill electrical and engineering series: Acoustics. New York, NY: McGraw – Hill.
- Blau, M., Sankowsky, T., Stirnemann, A., Oberdanner, H., & Schmitt, N. (2008). Acoustics of open fittings. Acoustics ’08, Paris, France.
- Fortune, T. W. (1997). Real ear compression ratios: The effects of venting and adaptive release time. American Journal of Audiology, 6, 55-63.
- Fuston, L. (2021, May 3). Comb Filtering: What Is It and Why Does It Matter? Sweetwater. https://www.sweetwater.com/insync/what-is-it-comb-filtering/
- Kochkin, S. (2010). MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. The Hearing Journal, 63(1), 19-20. https://doi.org/10.1097/01.hj.0000366912.40173.76
- Latzel, M. & Hobi, S. (2021) Receiver with mechanical vent provides benefit of open and closed acoustics for better speech understanding in noise and naturalness of own voice perception. Phonak Field Study News in preparation. Expected end 2021.
- Ricketts, T. (2000). Directivity quantification in hearing aids: Fitting and measurement effects. Ear and Hearing, 21(1), 45-58.
- Ricketts, T. A., Bentler, R., & Mueller, H. G. (2017). Essentials of modern hearing aids: Selection, Fitting, and verification. Plural Publishing.
- Winkler, A., Latzel, M., & Holube, I. (2016). Open versus closed hearing-aid fittings: A literature review of both Fitting approaches. Trends in
- Hearing, 20, 1-13. https://doi.org/10.1177/2331216516631741
- Woodward, J. (2018, October). New dual-path processing of vent loss compensation by Phonak enables a clear and rich sound quality when streaming.
- Phonak Insight. https://www.phonakpro.com/content/dam/phonakpro/gc_us/en/resources/evidence/white_paper/documents/audeo-marvel/Insight_BtB_Phonak_Marvel_vent_loss_compensation.pdf
Megan Adler, Au.D. is a Research Audiologist for Sonova U.S., located in Aurora, IL. She joined Sonova in 2008 and previously was part of the Customer Success Team as an Audiology Technical Support Representative. Her prior Audiology work history includes administering and interpreting audiological evaluations as well as hearing aid fitting and dispensing for adults and pediatrics at an Ear, Nose and Throat office. She earned her M.A. in Audiology at Northern Illinois University and Au.D. from Pennsylvania College of Optometry (now called Salus University).
David Taylor, Au.D. is a Research Audiologist for Sonova U.S., located in Aurora, IL. He joined Sonova in 2019. He earned a B.A. in Audio Arts & Acoustics at Columbia College Chicago, and Au.D. from Rush University.