
Getting Snug with the COSI: The Patient Expectations Worksheet (PEW)
Brian Taylor, Au.D.
The Client-Oriented Scale of Improvement (COSI) is probably the most popular outcome metric used in clinical audiology. For the unversed, the COSI asks the person with hearing loss, along with guidance from the clinician, to target and record up to five listening situations where hearing aids will provide benefit. Like other outcome measures, the COSI is first completed during a pre-fitting appointment before hearing aid use begins, and then re-assessed several weeks later in the aided condition. Developed by researchers at the National Acoustic Laboratories (Dillon, James & Gillis, 1997), the COSI captures two dimensions of outcome: final ability and degree of improvement, using a 5-point scale.
Much has been written about the COSI; see for example, pages 215-219 of the textbook, Essentials of Modern Hearing Aids. The focus of Clinical Bulletin #1 is using the COSI to gather information about patient expectations. As any experienced clinician knows, expectations can influence outcomes: Exceedingly high expectations can lead to disappointment, including returns for credit and non-use. In contrast, a patient with too low expectations, although easy to satisfy because their expectations are -ahem- low, nevertheless is not receiving the service and attention they deserve. For these reasons, the Patient Expectations Worksheet (PEW) is an easy and efficient way to align the individual’s expectations with final outcomes. The PEW was originally created by Palmer & Mormer (1999).
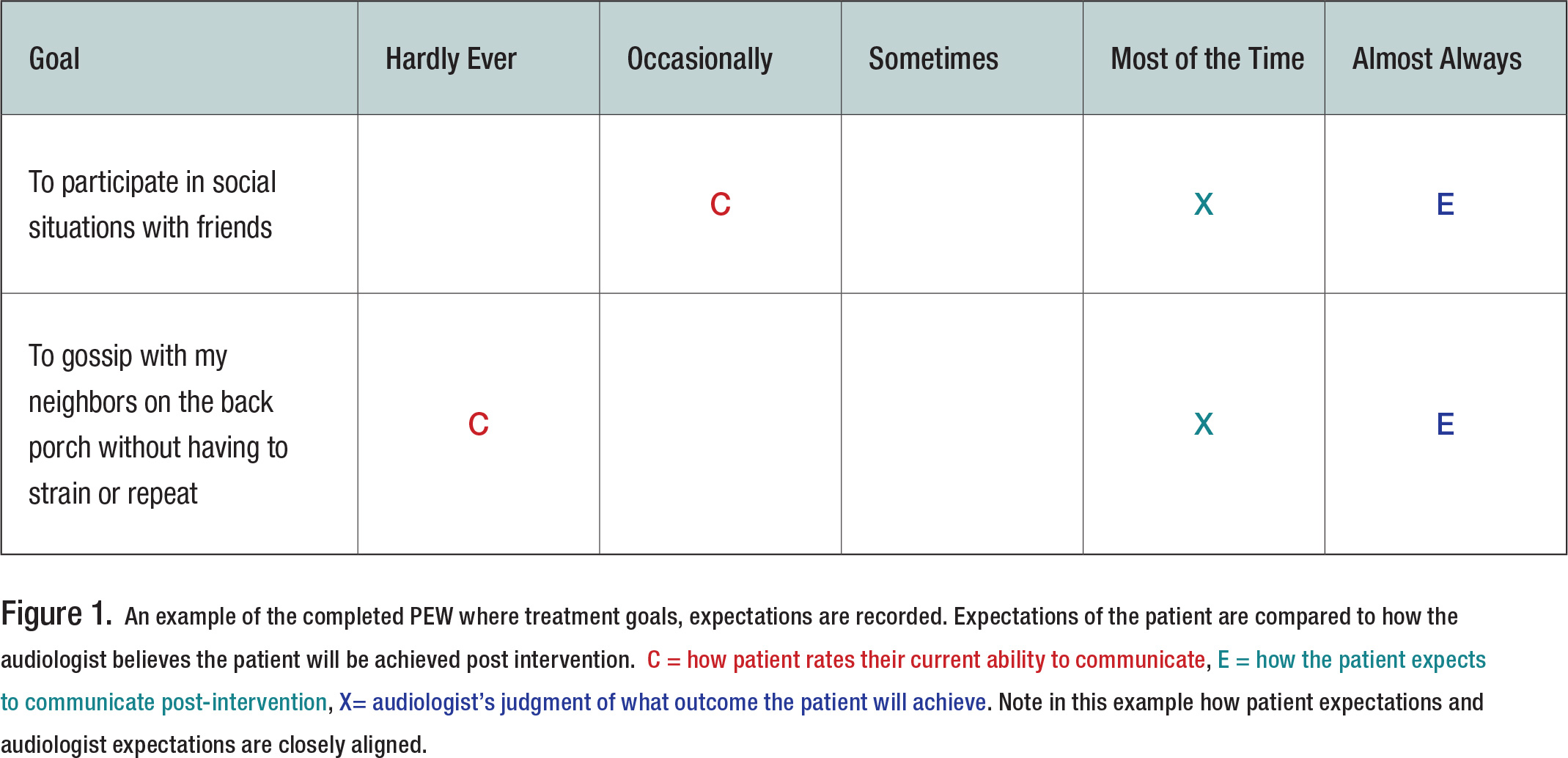
Here is how it works: As usual during the pre-fitting appointment, designate and record up to five goals on the COSI. In the example below, to keep it simple, there are just two goals listed. Next, after these goals have been recorded on the PEW, using the 1 to 5 scale, the patient indicates how often he is successful in the situation currently (C), prior to hearing aid use, and how he expects to function after the intervention (E). The “E” stands for expectations. Then, the audiologist marks the PEW with an X-mark (“x”) to indicate what she believes is a realistic expectation for that individual. The judgement of the clinician – where the “X” is placed for each goal – is based on the audiologic and non-audiologic information of that individual gathered during the pre-fitting appointment.
Assessing the individual’s self-reported functional communication ability and expectations using the 1 to 5 scale is an effective counseling tactic that helps establish the clinician as the trusted advisor. Figure 1 shows an example of a completed PEW in which the patient’s expectations and the audiologist’s judgments of success are fairly well aligned.
When Expectations are Out of Alignment
Occasionally the “E” of the patient and “X” of the clinician will not agree. In practical terms, this occurs when the “E” and “X” are separated by two or more categories. For example, the patient may state his expectations in the “almost always” category, while the clinician believes that realistic expectations fall in the “sometime” category. When expectations don’t align, the audiologist counsels the patient until he understands why his expectations might be too high or too low. Alternatively, when patient and clinician cannot align on expectations, a conversation about modifying the planned intervention must take place.
Determining Your “X”
A critical part of conducting the PEW is the clinician’s ability to determine or predict the outcome of each targeted goal on the 1 to 5 scale. This determination relies on sound clinical judgement and experience. However, the clinician should use the results of objective tests like the pure tone audiogram and Quick SIN, as well as familial support and the patient’s perceived attitude toward wearing hearing aids when deciding where to place the “X” on the 1 to 5 scale.
The Crux of the Matter
By allowing patients to weigh in on their post-fitting expectations and comparing those expectations to the clinician’s expectations of that patient, the PEW is an excellent vehicle for having a deeper, more person-centered dialogue about expected treatment outcomes. ■
References
- Dillon, H., James, A., & Ginis, J. (1997). Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. Journal of the American Academy of Audiology, 8(1), 27–43.
- Palmer, C. V., & Mormer, E. (1999). Goals and expectations of the hearing aid fitting. Trends in Amplification, 4(2), 61–71.
- Ricketts, T.A., Bentler, R.A., & Mueller, H.G. (2019). Essentials of modern hearing aids. San Diego: Plural Publishing.